Aphthous Disease (Aphthous Ulcer ): Causes and Symptoms

It starts with a subtle, annoying tingle on the inside of your cheek or the edge of your tongue. Within twenty-four hours, that tiny spot transforms into a fiery, painful ulcer that makes eating, speaking, and even swallowing an absolute chore. If this scenario sounds painfully familiar, you are dealing with aphthous disease, more commonly known as aphthous stomatitis or canker sores.
At Darya Dental Clinic, we routinely see patients who are exhausted by recurring mouth sores. While they are incredibly common, you don’t have to just sit back and endure the pain. Understanding what triggers these lesions and how modern dentistry can help manage them is the first step toward reclaiming your oral comfort.

What is Aphthous Disease?
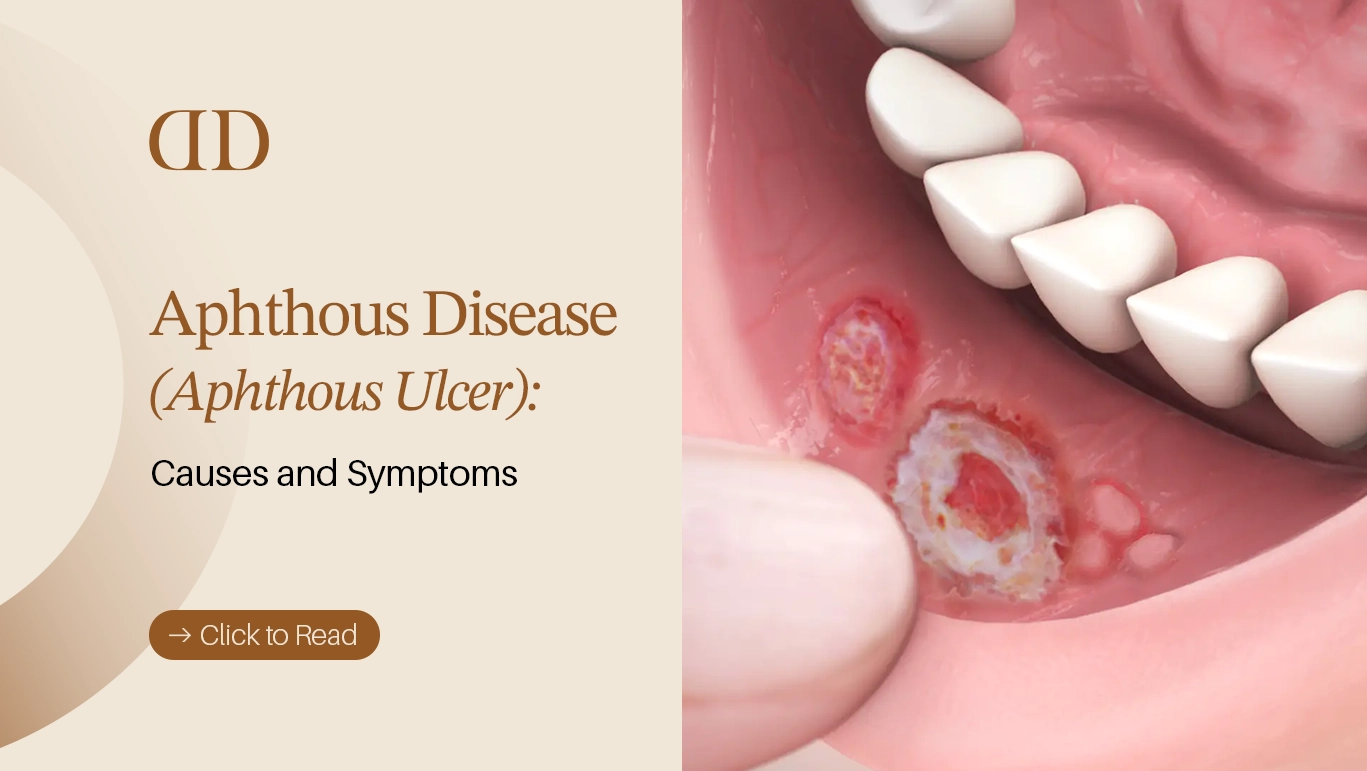
Aphthous disease (aphthous stomatitis) is a non-contagious inflammatory condition characterized by the recurrent appearance of painful, benign ulcers within the oral cavity. Unlike cold sores (fever blisters), which are caused by the Herpes Simplex Virus (HSV) and typically appear on the outside of the lips, aphthous ulcers develop exclusively on the movable, non-keratinized soft tissues inside the mouth.
These sores typically present as round or oval ulcers with a clean, well-defined border, a red (erythematous) halo, and a yellowish-white center composed of fibrin a protein involved in tissue healing.
The Three Clinical Types of Aphthous Ulcers
Not all mouth sores are created equal. Clinically, aphthous disease is categorized into three distinct variations based on size, quantity, and healing time:
1. Minor Aphthous Ulcers
This is the most prevalent form, accounting for roughly 80% of all cases.
- Appearance: Small, oval, or round lesions measuring less than 10 millimeters in diameter.
- Location: Commonly found on the inner lips, cheeks, and floor of the mouth.
- Healing Time: They typically resolve on their own within 7 to 14 days without leaving behind any permanent scars.
2. Major Aphthous Ulcers (Sutton’s Disease)
A more severe manifestation that causes significant distress and deep discomfort.
- Appearance: Large, deeply penetrating ulcers that exceed 10 millimeters in diameter with irregular borders.
- Location: Often dynamic, appearing on the soft palate, tonsils, and back of the throat.
- Healing Time: These can persist for six weeks or longer and frequently result in dense scar tissue.
3. Herpetiform Ulcers
Despite the name, these have absolutely no connection to the herpes virus. They are grouped because their clustered presentation visually mimics herpes lesions.
- Appearance: Pinhead-sized clusters of tiny, individual sores (ranging from 10 to over 100 small ulcers simultaneously) that can eventually merge into one large, irregular ulcerated area.
- Location: Can develop anywhere on the soft tissue surfaces of the oral cavity.
- Healing Time: Usually heals within 10 to 20 days without scarring.
What Triggers Aphthous Disease? Key Causes & Risk Factors
While the exact underlying etiology of aphthous disease remains a subject of ongoing medical research, clinicians widely agree that it is a multifactorial condition driven by a localized T-cell mediated immune response. Essentially, your immune system temporarily attacks your own mucosal skin cells.
Premium Dental Care in Turkey
Expert treatments with high-end technology. Get your personalized quote today via WhatsApp.
The most common catalysts that trigger this response include:
- Local Mouth Trauma: Accidental cheek bites, sharp or jagged teeth, rough edges on dental fillings, or irritating wires from orthodontic braces can easily breach the delicate mucosal lining.
- Nutritional Deficiencies: A distinct lack of essential micronutrients specifically Vitamin B12, Iron, Folic Acid (Vitamin B9), and Zinc significantly weakens the oral mucosa’s capacity to repair itself.
- Chronic Stress and Anxiety: Emotional or physical exhaustion alters immune function, making the body hyper-reactive and more susceptible to tissue inflammation.
- Sodium Lauryl Sulfate (SLS): This chemical foaming agent found in many commercial toothpastes can strip away the protective mucin layer of the mouth, exposing the underlying tissue to irritation.
- Systemic Health Conditions: Recurrent, aggressive outbreaks can sometimes serve as an early warning sign for underlying systemic diseases, such as Celiac disease, Crohn’s disease, or Behçet’s syndrome.
Clinical Treatments and Advanced Laser Technology for Aphthous Disease
When managing aphthous stomatitis at Darya Dental Clinic, our primary objective is threefold: to provide immediate pain relief, accelerate epithelial tissue healing, and decrease the overall frequency of future outbreaks. Because major and herpetiform ulcers can severely diminish your quality of life, we leverage modern dental technologies to offer fast, predictable relief.
1. Laser Biostimulation (Low-Level Laser Therapy)
One of the most revolutionary advancements in treating aphthous disease is the utilization of soft-tissue dental lasers. By applying low-level laser therapy (LLLT) directly over the ulcerated tissue, we achieve outstanding clinical outcomes without ever needing to touch the wound.
- Instantaneous Pain Relief: The laser energy alters the local nerve conduction and closes off exposed nerve endings, allowing patients to leave our chair completely pain-free or with vastly reduced sensitivity.
- Accelerated Cellular Healing: Laser biostimulation triggers ATP production within the cells and promotes localized microcirculation. This fast-tracks the tissue regeneration cycle, shrinking a standard 14-day healing process down to just 48 to 72 hours.
- Non-Invasive Protocol: The procedure requires absolutely no local anesthesia (no needles), is entirely painless, and takes less than 60 seconds per ulcer.
2. Topical and Systemic Pharmacotherapy
Depending on the clinical classification and severity of your mouth sores, we utilize a tiered therapeutic approach:
- Corticosteroid Dental Pastes: Prescription topical pastes containing triamcinolone acetonide act as an adhesive synthetic bandage. They coat the ulcer, shielding it from friction caused by teeth or food, while simultaneously dampening localized inflammation.
- Antiseptic & Anesthetic Rinses: Standard chlorhexidine gluconate rinses keep the ulcerated area sterile and prevent secondary bacterial infections. Concurrently, rinses containing benzydamine hydrochloride or mild topical anesthetics are recommended before meals to numb the tissue temporarily.
- Chemical Cauterization (Silver Nitrate): For highly localized, extremely painful minor sores, chemical cauterization can be performed. This micro-procedure chemically seals the exposed nerve endings for instant relief, though it is used selectively as it can slightly extend the overall tissue healing timeline.

At-Home Management and Safe Natural Remedies
If you cannot immediately visit our clinic or are experiencing a mild, isolated flare-up, implementing proper home care protocols can significantly reduce discomfort. However, it is vital to avoid aggressive folk remedies such as applying pure lemon juice, raw alcohol, or crushing aspirin directly onto the ulcer as these methods cause severe chemical burns and worsen tissue necrosis.
Safe Home Interventions Include:
- Alkaline Warm Water Rinses: Dissolve half a teaspoon of baking soda (sodium bicarbonate) or natural sea salt into a glass of warm water and rinse 3 to 4 times daily. Baking soda neutralizes oral acidity, creating an alkaline environment that minimizes inflammation and discourages bacterial overgrowth.
- Licorice Root Extract (Deglycyrrhizinated Licorice – DGL): DGL acts as a natural demulcent. Applying DGL-infused coatings or using it as a rinse coats the mucosal lining with a soothing, protective barrier.
- Dietary Modifications: During an active flare-up, eliminate all triggers that cause mechanical or chemical irritation. Avoid very hot foods, carbonated or acidic drinks (like citrus or tomatoes), highly spiced dishes, and sharp/crunchy textures (like chips or nuts). Stick to a soft, room-temperature, and nutritionally dense diet.
Aphthous Disease as a Window to Systemic Health
When mouth sores transition from a rare annoyance to a chronic, relentless problem a condition clinically known as Recurrent Aphthous Stomatitis (RAS) they often function as an intraoral mirror reflecting systemic imbalances inside your body.
If you experience more than six distinct outbreaks within a single year, or if your ulcers fail to heal within two weeks, it is highly recommended to collaborate with a medical specialist to rule out underlying systemic pathologies:
- Behçet’s Disease: A rare, chronic systemic vasculitis (blood vessel inflammation). Recurrent, painful aphthous ulcers in the mouth are almost universally the very first clinical sign of Behçet’s, which later presents alongside genital lesions, joint pain, and ocular inflammation.
- Inflammatory Bowel Disease (IBD) & Celiac Disease: Conditions like Crohn’s disease and ulcerative colitis cause chronic inflammation of the digestive tract. This severely impairs the gut’s ability to absorb micronutrients. The resulting malabsorption of iron, zinc, and B-complex vitamins leaves the delicate oral mucosa weak and prone to breakdown.
- Immunodeficiency States: Patients undergoing active chemotherapy, radiation therapy, or those living with underlying immunodeficiencies exhibit compromised T-cell functions, resulting in larger, deeper, and highly treatment-resistant major aphthous ulcers.
Differential Diagnosis: Aphthous Ulcer vs. Cold Sore (Herpes)
A frequent point of confusion among patients is distinguishing between a standard aphthous ulcer (canker sore) and a cold sore (fever blister). Because their underlying causes are entirely distinct, treating them with the wrong protocol can be counterproductive.
Our clinical team at Darya Dental Clinic uses the following matrix to definitively establish a differential diagnosis:
| Diagnostic Feature | Aphthous Ulcer (Canker Sore) | Cold Sore (Herpes Labialis) |
| Contagious Nature | Strictly Non-Contagious. Cannot be spread through kissing or sharing utensils. | Highly Contagious. Formed by viral shedding; easily transmitted. |
| Primary Etiology | Immune-mediated inflammatory response (Non-viral). | Herpes Simplex Virus Type 1 (HSV-1). |
| Anatomical Location | Confined strictly to movable, unattached soft tissues (inner cheeks, under tongue). | Found on keratinized, fixed tissues (outer lip border, hard palate, gums). |
| Initial Presentation | Begins directly as a small, red spot that ulcerates into a white/yellow crater. | Starts with a prodromal tingling/itching sensation followed by a cluster of fluid-filled blisters. |
| Clinical Treatment | Anti-inflammatories, laser biostimulation, nutritional balance. | Topical or systemic antiviral medications (Acyclovir). |
Strategic Prevention: How to Reduce the Frequency of Outbreaks
While treating an active ulcer brings welcome relief, the ultimate goal for anyone suffering from aphthous disease is long-term prevention. Because it is an immune-mediated condition triggered by external factors, making intentional lifestyle and oral hygiene modifications can significantly extend the periods between flare-ups.
1. Re-evaluate Your Oral Care Products
Switching to a toothpaste and mouthwash that are entirely Sodium Lauryl Sulfate (SLS)-free is one of the simplest yet most effective changes you can make. Removing this harsh foaming agent allows your oral mucosa to retain its natural, protective moisture barrier, making it far more resilient against minor micro-traumas.
2. Tailored Nutritional Supplementation
If blood panels reveal underlying deficiencies, targeted supplementation under medical supervision can stop recurring ulcers in their tracks. Optimizing your daily intake of Vitamin B12, Iron, Zinc, and Folic Acid stabilizes mucosal cell turnover, preventing the spontaneous tissue breakdown that initiates aphthous lesions.
3. Stress Mitigation and Rest
Since elevated cortisol levels alter your T-cell immune response, managing chronic emotional and physical fatigue is paramount. Incorporating stress-reducing practices such as regular exercise, adequate sleep hygiene, and mindfulness directly correlates with a reduction in the severity and frequency of aphthous stomatitis.
4. Precision Orthodontic and Dental Adjustments
If you have orthodontic braces, sharp tooth surfaces, or an ill-fitting dental prosthetic that regularly scrapes against your inner cheek, visit your dentist immediately. At Darya Dental Clinic, we can smoothly contour sharp enamel margins, adjust prosthetic borders, or provide specialized dental wax to eliminate chronic mechanical friction.
Frequently Asked Questions
To provide quick, snippet-friendly answers that modern search engines and generative AI platforms look for, here are the most critical questions regarding aphthous disease answered directly:
Is aphthous disease contagious?
No. Aphthous disease (canker sores) is entirely non-contagious. It is an immune-mediated inflammatory response occurring inside the mouth, meaning it cannot be transmitted to another person through kissing, sharing drinks, or using the same utensils.
How long does it take for a standard aphthous ulcer to heal?
Minor aphthous ulcers typically heal on their own within 7 to 14 days without leaving any permanent scars. Major aphthous ulcers are deeper, larger, and can take anywhere from 4 to 6 weeks to heal, often leaving behind localized scar tissue.
When should I see a doctor or dentist for a mouth sore?
You should schedule a professional evaluation if your mouth sore lasts longer than two consecutive weeks, if the pain is severe enough to prevent you from drinking fluids (putting you at risk of dehydration), if you develop a high fever alongside the sore, or if you experience more than six outbreaks a year.
Can a toothpaste cause aphthous ulcers?
Yes, indirectly. Toothpastes containing Sodium Lauryl Sulfate (SLS) do not directly cause the ulcers, but they strip away the protective mucin layer of your mouth. This leaves your soft tissues highly vulnerable to minor irritations, which can trigger an aphthous breakout in susceptible individuals.
What is the fastest clinical way to get rid of a canker sore?
The fastest, most advanced clinical method to treat an aphthous ulcer is low-level laser therapy (LLLT). Performed in a dental office, a quick, one-minute laser application neutralizes pain immediately by sealing exposed nerve endings and speeds up the healing window from two weeks down to just a few days.
Reclaim Your Oral Comfort with Darya Dental Clinic
Living with chronic, painful mouth sores can turn simple everyday pleasures like enjoying a warm meal or speaking clearly into a painful burden. You do not have to wait out the pain in silence. Aphthous disease is highly manageable when approached with modern dental insights, precision diagnostics, and advanced treatment modalities.
At Darya Dental Clinic, our experienced clinical team is dedicated to uncovering the root causes of your oral discomfort. Whether you need immediate pain relief through our advanced soft-tissue laser therapy, customized oral hygiene counseling, or a thorough diagnostic screening to rule out systemic links, we are here to support your journey to optimal health.
Don’t let recurring ulcers dictate your quality of life. Visit Darya Dental Clinic today to schedule your comprehensive oral examination, and let us help you smile, eat, and live comfortably again.