What Is Bone Grafting in Teeth?

If a dentist has ever told you that you’re “not a candidate” for implants due to jaw bone loss, the words bone grafting have probably come up along with a wave of questions you weren’t quite ready for. You’re in good company. Thousands of patients across Europe and the Middle East arrive at Darya Dental Clinic each year carrying exactly that uncertainty.
The good news is that bone loss in the jaw whether from a pulled tooth, gum disease, or years of wearing a denture is rarely the end of the road. Modern osseous regeneration techniques have made it possible to rebuild what was lost and restore the jaw to a state where it can support implants, prosthetics, or even neighbouring natural teeth. Understanding the process is the first step toward making an informed decision about your care.
What Is a Bone Graft and Why Does the Jaw Lose Bone in the First Place?
A bone graft is a surgical procedure in which a material derived from your own body, a donor, an animal source, or a synthetic compound is placed into a deficient area of the jaw to encourage the growth of new, native bone tissue. The graft itself does not become permanent bone; rather, it acts as a three-dimensional scaffold that your body’s own osteoblasts (bone-building cells) colonise and gradually replace with living bone over a period of months.
The term dental bone grafting is broad. Depending on the clinical situation, a surgeon may perform a socket preservation graft (placed immediately after extraction), a sinus lift (to augment the upper posterior jaw beneath the sinus floor), a ridge augmentation (to widen or heighten a thin jaw ridge), or a block graft (transplanting a solid piece of bone, usually from the chin or jaw angle). Each technique addresses a slightly different anatomical challenge.
As for why bone disappears: the jawbone is biologically active and responds directly to mechanical stimulation. When a tooth root is present, chewing forces travel through it into the surrounding bone, signalling the body to maintain density there. Remove the tooth, and that signal vanishes. Research cited by the American Academy of Periodontology (www.perio.org) indicates that up to 40–60% of alveolar bone volume can be lost within the first year after a tooth is removed a process called resorption. Periodontal disease accelerates this further, attacking the bone directly through bacterial inflammation.
Who Needs a Bone Graft?
Not every extraction or case of gum disease leads to a grafting procedure but several clinical scenarios make osseous augmentation either strongly advisable or medically necessary.
- After tooth extraction: A tooth bone graft placed at the time of extraction dramatically slows the resorption process, keeping the site viable for a future implant.
- Before implant placement: A bone graft for dental implants is often a prerequisite when the residual ridge is too thin or shallow to anchor a titanium fixture reliably.
- Periodontal disease: Advanced gum disease destroys the bone supporting existing teeth. Osseous regeneration can help stabilise them and arrest further deterioration.
- Facial trauma or tumours: Accidents, cysts, or benign jaw lesions can leave irregular voids that require reconstruction before any prosthetic treatment.
- Long-term denture wearers: Years of denture pressure against gum tissue frequently cause significant ridge resorption, making grafting a common preparatory step before converting to implant-retained prosthetics.
What Does a Bone Graft Look Like? Graft Materials Explained
Before surgery, patients often want to understand what is actually being placed inside their jaw. Graft materials are broadly classified into four categories, each with its own biological rationale and track record.
| Graft Type | Source | Key Advantage | Consideration |
|---|---|---|---|
| Autograft | Patient’s own body (chin, jaw ramus, hip) | Highest biological compatibility; contains living cells | Requires a second surgical site |
| Allograft | Processed cadaveric human donor bone | No second surgical site; widely available | Rigorous processing to eliminate disease risk |
| Xenograft | Animal bone (typically bovine) mineral | Excellent long-term resorption profile | Animal-derived; some patients decline on ethical grounds |
| Alloplast | Synthetic (hydroxyapatite, calcium phosphate) | No disease transmission; consistent quality | No living cells; purely osteoconductive |
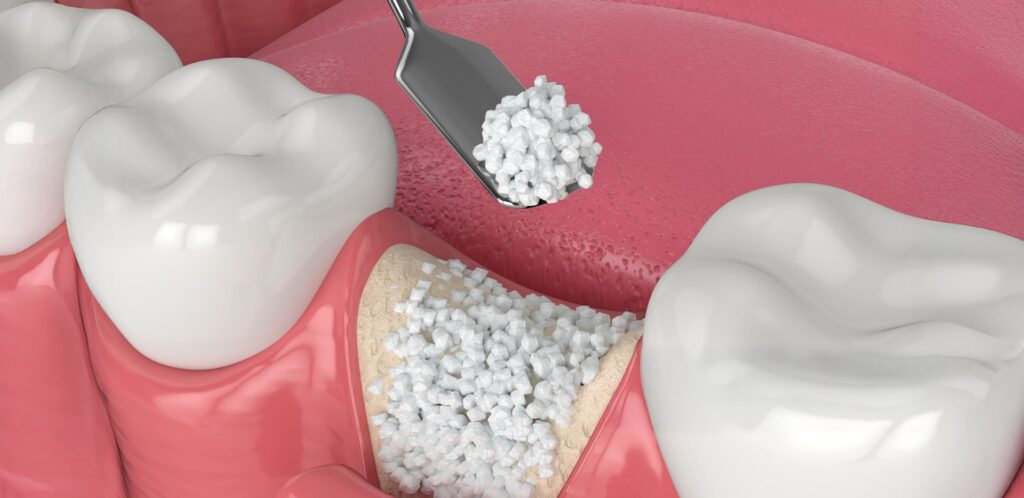
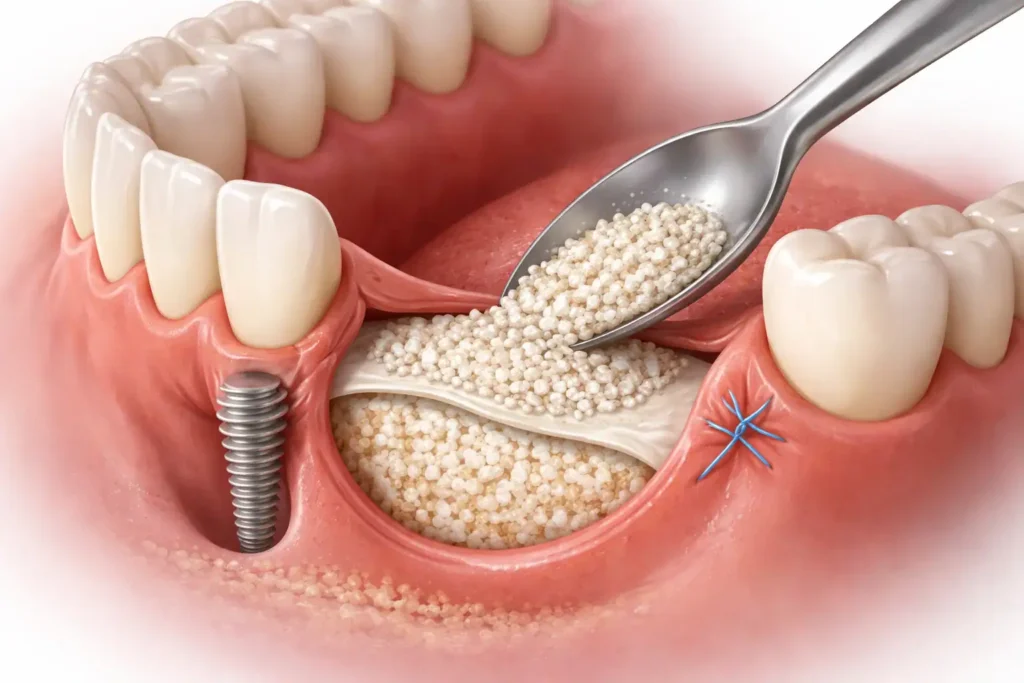
In particulate form, the graft material typically resembles fine, off-white granules similar in appearance to coarse salt. In block form (used for larger defects), it is a solid piece shaped to fit the defect and secured with small titanium screws. Over the graft, surgeons often place a resorbable collagen membrane that acts as a physical barrier, preventing the faster-growing soft tissue cells from invading the space where bone should form. This technique is called Guided Bone Regeneration (GBR).
Is Bone Grafting Painful? An Honest, Nuanced Answer
Intraoperatively, bone grafting is performed under local anaesthesia often combined with sedation for anxious patients so there is no pain during the procedure itself. What varies considerably is the post-operative experience, which depends on the size and location of the graft, the technique used, and the individual patient’s physiology.
Premium Dental Care in Turkey
Expert treatments with high-end technology. Get your personalized quote today via WhatsApp.
A straightforward socket preservation after a single extraction is typically managed with standard over-the-counter analgesics and mild discomfort that peaks at 48–72 hours. A bilateral sinus lift or a block graft harvested from the hip, on the other hand, constitutes a more involved surgery with a correspondingly longer and more noticeable recovery period. Most patients report that the experience was considerably more manageable than they had anticipated particularly when post-operative instructions were followed carefully.
A useful perspective: Many patients describe tooth extraction as more acutely uncomfortable than the grafting procedure that follows it. The graft site is typically well-covered with soft tissue, and modern anaesthetic techniques make the procedure itself essentially pain-free. The first two to three post-operative days are the most physically demanding part of the journey.
Dental Bone Graft Healing Stages: A Realistic Week-by-Week Timeline
Understanding the biology of osseous regeneration helps patients set accurate expectations and interpret what they observe during recovery. The process unfolds in overlapping but distinct phases here is a practical breakdown of what typically happens and when.
Days 1–3 Haemostasis & Inflammation
Swelling and bruising typically peak within the first 48–72 hours. A blood clot forms over the graft this is critical and must not be disturbed. Cold compresses applied intermittently (20 minutes on, 20 minutes off) can meaningfully reduce facial swelling. Most patients require 2–3 days away from regular activities.
Days 4–14 Early Soft Tissue Repair
Granulation tissue begins forming around the graft material. Tenderness decreases considerably for most patients. Sutures (if non-dissolving) are typically removed around day 7–10. Oral hygiene resumes carefully around the graft site.
Weeks 3–8 Vascularisation & Bone Formation
New blood vessels infiltrate the graft scaffold a process called angiogenesis. Osteoblasts begin laying down an organic bone matrix (osteoid). This phase is invisible from the outside but is where the most crucial biological work occurs.
Months 3–6 Mineralisation & Consolidation
The osteoid calcifies and begins to mineralise into mature lamellar bone. Updated CBCT (cone beam) imaging is typically taken at this stage to assess whether the graft has integrated sufficiently for implant placement.
Month 6+ Full Maturation
The regenerated bone continues to remodel and strengthen. Implant placement typically follows at this point, where clinically indicated. Factors like smoking, systemic health, or nutritional deficiencies can significantly influence this timeline.
The overall duration from graft placement to implant readiness generally falls between four and nine months, though smaller socket preservation grafts can sometimes allow implant placement as early as three months. Your surgical team’s imaging assessment not a fixed calendar date is the definitive guide.
How to Speed Up Bone Graft Healing: Evidence-Informed Strategies
You cannot accelerate biology on a cellular level, but you can create the optimal environment for your body’s natural healing mechanisms. The following approaches are supported by clinical evidence and are routinely recommended by oral and maxillofacial surgeons.
- Prioritise dietary protein. Bone matrix is largely made of collagen, which requires amino acids. Eggs, fish, lean poultry, legumes, and dairy should feature prominently in the weeks following surgery.
- Maintain scrupulous but gentle oral hygiene. Bacteria are the primary threat to graft survival. Use any prescribed chlorhexidine rinse as directed, brushing carefully around (never directly on) the surgical site.
- Eliminate smoking entirely. Nicotine causes vasoconstriction, reducing blood flow to healing tissue. The American Association of Oral and Maxillofacial Surgeons (www.aaoms.org) identifies smoking as one of the leading risk factors for dental bone graft failure. Even light smoking meaningfully compromises outcomes.
- Avoid alcohol for at least the first two weeks. Alcohol interferes with blood clot stability, immune function, and the pharmacokinetics of any prescribed antibiotics.
- Delay strenuous exercise. Elevated blood pressure and heart rate from vigorous exercise can disrupt the graft site in the first 7–10 days. Light walking is generally acceptable after 48–72 hours; contact sports and heavy weight training should wait until cleared by your surgeon.
- Attend every follow-up appointment. Early detection of infection, membrane exposure, or partial graft displacement allows for prompt intervention dramatically improving the chance of successful integration.
Vitamin D and calcium adequacy also play a supporting role in bone mineralisation. If you have reason to suspect deficiency in either (which is common at northern latitudes and among older adults), a conversation with your general practitioner before surgery is worthwhile.
Can a Bone Graft Fall Out? Recognising and Responding to Complications
A small amount of graft granules appearing at the wound surface during the first few days is not automatically a cause for alarm particularly with particulate grafts, where the granules are loose by nature. However, several signs warrant prompt contact with your clinic.
- Visible white or greyish material emerging from the wound in significant or increasing quantities.
- A protective membrane that appears to be lifting from the gum tissue or protruding into the oral cavity.
- Persistent or intensifying pain beyond the first week, rather than a gradual improvement.
- Signs of localised infection: swelling that worsens rather than subsides, fever, bad taste, or visible pus.
- A sensation of exposed, dry bone in the socket though dry socket is less common when a graft is placed, it can still occur in some cases.
Regarding the membrane: if it begins to come out prematurely, do not attempt to push it back or remove it yourself. Contact your dental provider for assessment. Early membrane loss does not automatically mean the graft has failed but it does require clinical evaluation to determine whether intervention is needed.
Important note on “failed” grafts: Images you may find online of failed dental bone graft healing pictures often represent extreme or poorly managed cases. With careful surgical technique, appropriate patient selection, and diligent aftercare, the clinical success rate of modern bone grafting procedures is generally reported to be high in the peer-reviewed literature though individual outcomes always vary.
How Much Is a Bone Graft? Understanding the Cost Landscape
Dental bone graft cost varies considerably based on geography, the type and volume of graft material used, whether a membrane is required, the complexity of the case (a sinus lift is more involved and more expensive than a simple socket graft), and whether the procedure is performed by a specialist periodontist or oral surgeon versus a general dentist.
In Western Europe and North America, bone graft dental cost for a single-site socket preservation typically ranges from several hundred to well over a thousand euros or dollars. More extensive procedures such as bilateral sinus lifts can rise substantially further. In Turkey, where Darya Dental Clinic operates, the combination of lower operational costs, competitive lab fees, and a highly trained specialist workforce means that comparable procedures are often available at a fraction of the price patients would pay at home without any compromise in the materials used or the clinical standards applied.
Patients who are considering dental tourism for bone grafting for dental implants should factor in travel and accommodation alongside treatment costs, and ensure they have a clear plan for any follow-up care needed once they return home. Darya Dental Clinic provides detailed treatment plans in advance, including all costs, so there are no surprises.
Frequently Asked Questions About Bone Grafting
When can I eat solid food after a bone graft?
Most patients transition through three dietary stages. For the first 24–48 hours, cold or room-temperature liquids and very soft foods (yoghurt, smoothies, mashed potato) are recommended. From day 3 to approximately day 14, soft foods that require minimal chewing scrambled eggs, soft fish, pasta are generally tolerable. Solid foods that require significant bite force are typically reintroduced gradually from weeks 2–4 onward, depending on how well healing is progressing.
How long does a bone graft last without an implant?
A successfully integrated graft becomes genuine native bone it is not a temporary filling. However, without the mechanical stimulation that a tooth root or implant provides, the surrounding jaw will gradually resume its natural resorption process over time. The benefit of the graft is therefore best preserved by proceeding to implant placement within a clinically appropriate window.
Can you get dry socket with a bone graft?
Dry socket is less common when a graft is placed immediately after extraction, because the graft material itself helps stabilise the socket. However, it is not impossible. Smoking, rinsing forcefully, using straws, or eating on the surgical side in the first few days all increase the risk. If you experience worsening pain and a bad odour from the socket from around day 3–4, contact your clinic promptly.
When can I exercise after a dental bone graft?
Light activity gentle walking is typically fine after 48–72 hours. Activities that significantly elevate blood pressure and heart rate are generally discouraged for at least 7–10 days. Contact sports, heavy resistance training, and anything involving impact or straining should wait until you have specific clearance from your surgeon.
How long does it take to heal before an implant can be placed?
The most accurate answer is: when your CBCT scan confirms sufficient bone density and volume not on a fixed calendar date. As a general guide, small socket preservation grafts in ideal patients can allow implant placement from around 3–4 months post-graft. Larger augmentations typically require 6–9 months or occasionally longer.
Closing Perspective: Bone Grafting as the Foundation of a Lasting Smile
Bone grafting is, in many ways, the unsung hero of modern implant dentistry. It rarely gets the attention that the implant or the crown above it receives yet without adequate bone architecture, neither of those treatments is possible. For patients who have been told they lack the bone for implants, an osseous augmentation procedure is not a complication or a detour. It is, more accurately, the beginning of a viable path.
The science behind grafting bone has advanced enormously over the past two decades. Graft materials are better characterised, surgical techniques are more refined, and the understanding of guided bone regeneration continues to evolve. None of this translates into a trivial procedure it is still surgery, and it still requires time to heal. But for those who complete the process carefully, the outcome is a jaw that can support lasting restorations and a quality of life that bone loss had threatened to curtail.
If you have been given reason to explore this option or if you suspect bone loss may be a factor in your own case the most important next step is a thorough consultation that includes three-dimensional imaging. At Darya Dental Clinic, patients receive a complete diagnostic workup before any treatment plan is proposed, so that recommendations are grounded in your specific anatomy rather than assumptions. Visit us at daryadentalturkey.com to book a free consultation.